Preventing Suicide in Adolescents
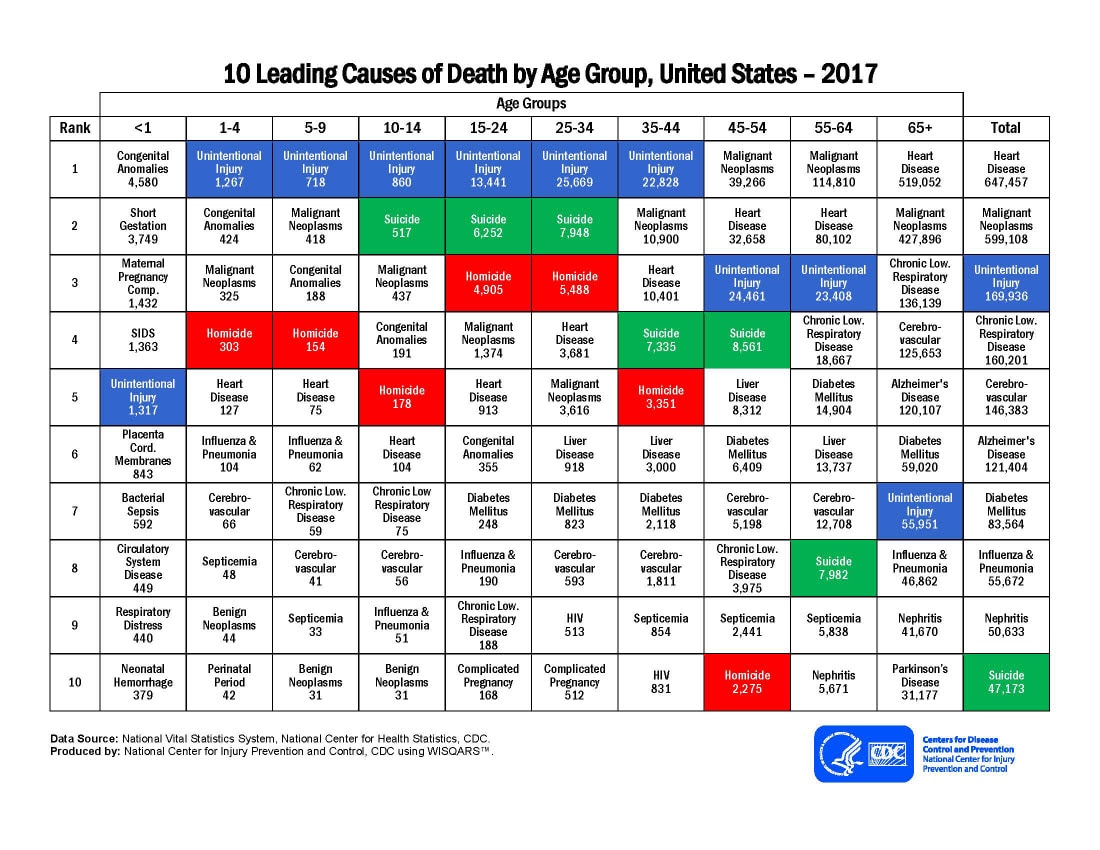
Suicide in children is a currently a major public health issue. According to the CDC, as of 2017, suicide is the number 2 cause of death in age groups between 10-34 (1). Suicide rates among adolescents rose sharply between 2007-2017, with a total 50% increase in suicide rates over 10 years. Additionally, the rate of suicide increased more drastically between 2012-2017 (about 7% increase per year) than it did between 2007-2012 (about 3% increase per year), further demonstrating that there has been a steep recent increase in suicide rates among children and adolescents (2). Risk of suicide in adolescents has been strongly linked to mental illness, and studies show that 90% of people who have committed suicide suffered from at least one mental disorder (3).
Risk of suicide in adolescents is often associated with mental illness, especially depressive symptoms. In a study performed in Brazil, adolescents from various schools were tested for depressive symptoms and suicide risk. The study found that there was a higher percentage of suicide amongst adolescents who screened positively for depression than in adolescents who screened negatively for depression (4). Moreover, a retrospective cohort longitudinal study done on adolescents looked at symptoms during childhood and their effects on later risk of suicide. It found that those who exhibited symptoms of depression during childhood, including irritability, a frequently observed symptom of childhood depression, had a significantly greater risk of suicidality in adolescence (5).
Other mental disorders have also been linked to mental illness, including mood disorders and anxiety disorders. A longitudinal systematic review and meta-analysis which looked at all mental disorders found that only specific affective disorders, such as bipolar disease, anxiety disorder, and depression, are positively associated with suicide attempts. Furthermore, results found that psychiatric comorbidity, having more than one mental disorder, had a very strong positive association with suicide risk (6).
Studies also show a link between risky behaviors and both depressive symptoms and suicide risk in adolescents. According to one study, teens who engaged in illicit substance use, smoking, and sexual activity were at significantly increased odds for depression and risk of both suicide ideation and attempts (7). Another study, which looked at substance use, tobacco use, and marijuana use, found similar results (8). In a third study, participants reported their use of alcohol, cigarettes, ketamine, and MDMA during the past year, as well as their suicidal ideation and attempts. Results of the study found that use of any of these substances was correlated with increased suicidal behavior (9).
Difficulty at home and lack of parental support can also be a key contributing factor to suicide risk in adolescents. One study found that adolescents who experienced family conflict at home or had negative relationships with their parents had an increased risk of both depression and suicide (8). Another study found that children of parents who never or rarely told them they were proud of them, that they did a good job, or helped them with their homework, had the highest risk of suicide, especially at younger ages (10). A third study similarly found that perceptions of low parental support were an independent risk factor for attempted suicide in adolescents (11).
Various issues at school, including academic issues and social issues, such as bullying, are also associated with increased risk of suicide in adolescents. A study that looked at depressed adolescents found that those who repeated a grade in school had an increased risk of suicide (8). Furthermore, in a study conducted in Mexico on middle and high school students, higher number of failed courses and lower self-perceived academic performance were associated with increased risk of suicide attempt (12). Moreover, bullying victimization is a major risk factor for suicide. A study conducted using a sample of pediatric patients screened for mental illness found that all types of bullying were positively associated with suicide risk, and verbal bullying was associated with the greatest suicide risk. It also found that that the risk of suicide was greater when bullied patients were also depressed (13). Similarly, another study performed on pediatric emergency room patients found that those who reported recently being a victim of bullying had a significantly greater chance of screening positively for suicide risk (14). Bullying can cause social isolation, as well as feelings of lowliness and worthlessness, which can in turn lead to depression and risk of suicide.
Social support can be a protective factor against suicide risk. A study which interviewed adolescents about mental health issues, suicidal behavior, and quality of relationships found that friendship positivity, sibling relationship positivity, family cohesion, maternal and paternal care were inversely related with risk of suicide (15). Another study likewise demonstrated that social support from parents, classmates, and close friends served as a buffer for the relationship between depression and suicide risk (16).
There are certain common factors that are hypothesized to lead to suicide. One study, which was a systematic review of risk factors, found that hopelessness and previous suicide attempts were the main risk factors for suicide (17). Another study, in describing the correlation between mental disorders and suicide, explained that this association is due to a factor which is common to most disorders, like an experience of distress or impairment (18). These feelings are often effects of the various factors outlined, which can explain the association between these issues and increased suicide risk.
Nevertheless, America’s battle against adolescent suicide is not hopeless. With a two-pronged plan involving an emphasis on preventative measures and on consistent screening for mental disorders, America can combat this “suicide epidemic.” Training parents and teachers in the detection of symptoms of depression, such as feelings of helplessness and worthlessness, enables them to identify at-risk teens and provide them with the counseling and assistance they need. Parents need to be aware of potential substance abuse, as well as ensuring that they maintain strong bonds with their children and create a safe space for them to express concerns and emotions. Schools should increase education regarding bullying, create compelling initiatives to decrease it, and impose harsh consequences for bullies themselves. Additionally, teachers and administrators should attempt to build the self-esteem of each student, thereby enabling them to face struggles and challenges without the risk of falling into depression. The second prong involves increased screening in schools for depression, feelings of helplessness, mood disorders, low self-esteem, and other high risk factors for suicide.
This plan is a strong one because it would increase overall education regarding mental health and suicide prevention among educators, parents, and children, and would enable many to detect risk factors from their onset. Furthermore, it would decrease the prevalence of risk factors and build strong support systems for adolescents to turn to in times of need. However, this plan is not without faults. This program relies on the voluntary education of adults, and on a will for behavioral change. It does not guarantee that parents will take the steps necessary to build an accepting environment, nor that teachers and administrators will shift their focus from increasing standardized test scores to building mentally healthy adolescents. Furthermore, not every student can undergo in school screening, especially in schools in impoverished areas with already deficient budgets.
Though this plan has potential downfalls, it’s likely benefits are stronger, and it should be implemented presently to ensure the decrease in suicide prevalence and the protection of the lives of innocent adolescents.
Sources:
1) https://www.cdc.gov/injury/images/lc-charts/leading_causes_of_death_by_age_group_2017_1100w850h.jpg
{kind=link}
2) Curtin SC, Heron M. Death rates due to suicide and homicide among persons aged 10–24: United States, 2000–2017. NCHS Data Brief, no 352. Hyattsville, MD: National Center for Health Statistics. 2019.
3) Bilsen, J. (2018). Suicide and youth: risk factors. Frontiers in psychiatry, 9, 540.
4) de Araújo Veras, J. L., Ximenes, R. C. C., de Vasconcelos, F. M. N., & Sougey, E. B. (2016). Prevalence of suicide risk among adolescents with depressive symptoms. Archives of psychiatric nursing, 30(1), 2-6.
5) Orri, M., Galera, C., Turecki, G., Forte, A., Renaud, J., Boivin, M., … & Geoffroy, M. C. (2018). Association of childhood irritability and depressive/anxious mood profiles with adolescent suicidal ideation and attempts. JAMA psychiatry, 75(5), 465-473.
6) Gili, M., Castellví, P., Vives, M., de la Torre-Luque, A., Almenara, J., Blasco, M. J., … & Lagares, C. (2019). Mental disorders as risk factors for suicidal behavior in young people: A meta-analysis and systematic review of longitudinal studies. Journal of affective disorders, 245, 152-162.
7) Hallfors, D. D., Waller, M. W., Ford, C. A., Halpern, C. T., Brodish, P. H., & Iritani, B. (2004). Adolescent depression and suicide risk: association with sex and drug behavior. American journal of preventive medicine, 27(3), 224-231.
8) Consoli, A., Peyre, H., Speranza, M., Hassler, C., Falissard, B., Touchette, E., … & Révah-Lévy, A. (2013). Suicidal behaviors in depressed adolescents: role of perceived relationships in the family. Child and adolescent psychiatry and mental health, 7(1), 8.
9) Wang, P. W., & Yen, C. F. (2017). Adolescent substance use behavior and suicidal behavior for boys and girls: a cross-sectional study by latent analysis approach. BMC psychiatry, 17(1), 392.
10) King, K. A., Vidourek, R. A., Yockey, R. A., & Merianos, A. L. (2018). Impact of parenting behaviors on adolescent suicide based on age of adolescent. Journal of Child and Family Studies, 27(12), 4083-4090.
11) Miller, A. B., Esposito-Smythers, C., & Leichtweis, R. N. (2015). Role of social support in adolescent suicidal ideation and suicide attempts. Journal of Adolescent Health, 56(3), 286-292.
12) Orozco, R., Benjet, C., Borges, G., Arce, M. F. M., Ito, D. F., Fleiz, C., & Villatoro, J. A. (2018). Association between attempted suicide and academic performance indicators among middle and high school students in Mexico: results from a national survey. Child and adolescent psychiatry and mental health, 12(1), 9.
13) Kodish, T., Herres, J., Shearer, A., Atte, T., Fein, J., & Diamond, G. (2016). Bullying, depression, and suicide risk in a pediatric primary care sample. Crisis.
14) Stanley, I. H., Horowitz, L. M., Bridge, J. A., Wharff, E. A., & Teach, S. J. (2016). Bullying and suicide risk among pediatric emergency department patients. Pediatric emergency care, 32(6), 347.
15) Van Meter, A. R., Paksarian, D., & Merikangas, K. R. (2019). Social functioning and suicide risk in a community sample of adolescents. Journal of Clinical Child & Adolescent Psychology, 48(2), 273-287.
16) Fredrick, S. S., Demaray, M. K., Malecki, C. K., & Dorio, N. B. (2018). Can social support buffer the association between depression and suicidal ideation in adolescent boys and girls?. Psychology in the Schools, 55(5), 490-505.
17) Hawton, K., Sutton, L., Haw, C., Sinclair, J., & Harriss, L. (2005). Suicide and attempted suicide in bipolar disorder: a systematic review of risk factors. The Journal of clinical psychiatry.
18) Nock, M. K., Hwang, I., Sampson, N. A., & Kessler, R. C. (2010). Mental disorders, comorbidity and suicidal behavior: results from the National Comorbidity Survey Replication. Molecular psychiatry, 15(8), 868-876.

This entry is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International license.